From Insight to Impact: CGM's Journey to the Mainstream
May 01, 2024
In the landscape of diabetes management, Continuous Glucose Monitors (CGMs) have revolutionized the approach to monitoring glucose levels, offering both patients and healthcare professionals a dynamic tool to manage diabetes more effectively.
Recent studies and presentations at ATTD2024 have highlighted the multifaceted benefits of CGM systems, ranging from their impact on reducing mortality among insulin-dependent diabetes patients to their emerging use in populations not traditionally considered for such intensive monitoring.
In this blogpost we focus on recent insights about the use of CGMs in people with diabetes.
- First-ever CGM Mortality Data
- CGM for People with Diabetes Not On Insulin
- Proposed Use of CGM for People with Type 2 Diabetes
1. First-ever CGM mortality data

That glucose sensors provide added value for people with diabetes who use insulin is already known.
However, most studies focus on improving glucose control, reducing hypoglycemia and hyperglycemia, and the quality of life of individuals using such sensors.
At ATTD2024, prof dr Peter Raeven (University of Arizona, US) presented the first-ever mortality data about CGM use.
Within the Veterans Affairs records, he searched for people with type 1 and type 2 diabetes on insulin, who started a CGM between 2015 and 2020, and looked at the long-term effects of CGM-use, focusing on all-cause mortality.
The Veteran Affairs Healthcare System data reflects data from more than 10 million non-active veterans from all over the US, spanning across more than 1300 faciilities.
It's important to note that CGM is covered for US veterans who use more than 3 injections of insulin per day, or who use an insulin pump.
He identified a really large cohort:
- 7513 people with type 1 diabetes, of whom 4 590 started a CGM between 2015-2020,
- and 38 553 people with type 2 diabetes, of whom 13 373 started a CGM between 2015-2020.
The method of this retrospective observational cohort study was similar as in his previous publication (Diabetes Care 2023), where he found that the use of CGM in people with diabetes on insulin leads to a greater drop in HbA1c than in nonusers in 12 months (-0.26% for people with type 1 diabetes and 0.35% for people with type 2 diabetes).
The data showed that the mortality rate of people with diabetes on insulin using a CGM was significantly lower than those with diabetes not on CGM.
- Although the positive effect on mortality was higher in people with type 1 diabetes (hazard ratio of 0.43 = 57% lower risk),
- there was also a significant positive effect in people with type 2 diabetes (hazard ratio of 0.86 = 14% lower risk).
The curves separated early in the treatment with a CGM and continued over 18 months,
and the results stayed robust to many sensitivity analysis.
In a subset analysis they also investigated the causes of death and differentiated between all-cause mortality, cardiovascular death and non-cardiovascular death.
- The data showed a similar effect on all types of death for people with type 1 diabetes.
- For people with type 2 diabetes, the mortality reductions seemed to be more pronounced for non-cardiovascular death than for cardiovascular death.
This data, derived from a comprehensive analysis of health records from the Phoenix VA Health Care System, confirms the life-saving potential of CGM technology.
Both type 1 and type 2 diabetes patients on insulin therapy showed highly significant reduced mortality rates when using CGM systems.
This is an essential development, reinforcing CGM as not just a tool for managing glucose levels but as a critical component in extending the lives of patients with diabetes.
Dr Raevan pointed out that in this cohort of people with diabetes on insulin the number needed to treat over 18 months to prevent one death
- was 30 for people with type 1 diabetes
- and 77 for people with type 2 diabetes on insulin.
By comparison: for statins, the number needed to treat over 18 months to prevent one death in these high-risk individuals, ranges from 50 to 130 over 5 years.
2. CGM for People with Diabetes Not on Insulin
The landscape of continuous glucose monitoring (CGM) for diabetes management is rapidly evolving, extending beyond its traditional use in individuals on intensive insulin therapy.
While CGM has long been a cornerstone in managing blood glucose levels for those on intensive insulin regimens, recent developments highlight its expanding role, particularly in people with diabetes not on insulin.
Recent research and presentations at conferences like ATTD2024 shed light on this paradigm shift:
- A systematic review by Jancev et al. (Diabetologia 2024) compared CGM with self-monitoring blood glucose (SMBG) across 12 randomized controlled trials involving individuals with type 2 diabetes. Their findings revealed a comparable reduction in HbA1c (-3.43 mmol/mol) among participants using insulin or oral agents alone. (See picture here.)
- Aleppo et al. (Diabetes Technol Ther 2023) provided insights from a narrative review, summarizing evidence from various studies investigating CGM use in people with type 2 diabetes treated solely with basal insulin or non-insulin therapies. Their review underscores the rationale for expanding CGM access in this demographic. (See picture here)
- Dexcom presented data at ATTD2024, analyzing 941 individuals with type 2 diabetes who initiated Dexcom sensors. Results showcased improvements in HbA1c across all groups, including those on intensive insulin therapy (n=735, HbA1c 8.5% > 7.8%), basal insulin alone (n=65, HbA1c 8.7% > 7.7%), and no insulin (n=141, HbA1c 8.1% >7.3%). (See picture here)
- Abbott's subanalysis of the RELIEF trial (real-World Evidence of FreeStyle Libre) at ATTD2024 revealed a 65% reduction in acute diabetes complications among 1272 individuals not on insulin but on sulfonylurea therapy following FreeStyle Libre sensor initiation, in the year following the initiation of a FreeStyle Libre sensor compared to the previous year (7.2% > 2.5%). (See picture here)
- Dr. Lanzinger's (Ulm University, Germany) presentation at ATTD2024, drawing from the Diabetes Prospective Follow-up Registry, highlighted HbA1c improvements among 2561 adults with type 2 diabetes using CGM. Of this cohort, 37% were on basal-bolus therapy, 15% on basal insulin alone, and 48% on non-insulin regimens. 6 months after CGM initiation, HbA1c dropped significantly over all groups (basal-bolus therapy: 7.5% > 7.3%, basal-only: 7.2% >6.8%, non-insullin users: 6.9%> 6.8%). (See picture here)
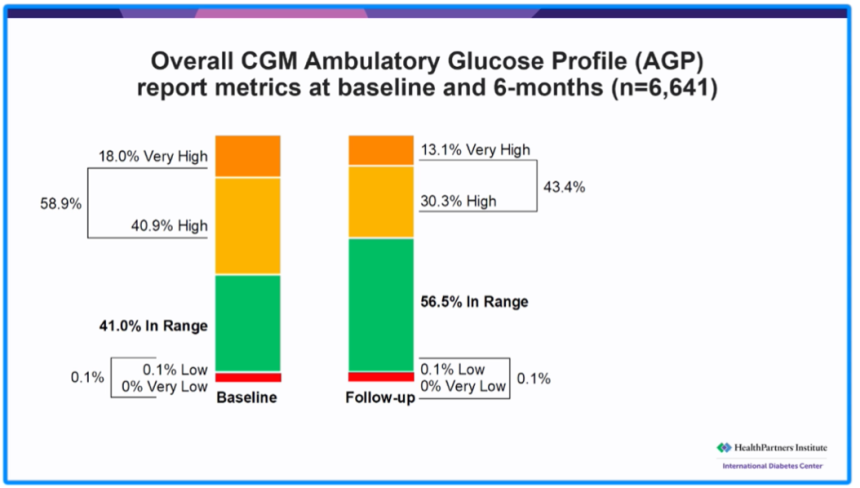
- Additionally, Dr. Bergenstal's (International Diabetes Center, US) real-world CGM outcomes presented at ATTD2024 showcased promising results among 6641 individuals with type 2 diabetes not on insulin. Initiation of a Dexcom G6 sensor led to significant improvements in Time In Range (41% > 57%) and GMI or estimated HbA1c (8.1% > 7.7%). (See picture here)
While the reduction in HbA1c varies considerably across studies, collectively, they demonstrate that initiating CGM has a substantial positive impact on overall glucose control in people with diabetes not on insulin.
As the cost of CGMs is decreasing, let's hope that one day continuous use of CGM will become cost-effective for all individuals with diabetes, not just those using insulin.
3. Proposed use of CGM for people with type 2 diabetes

Based on the mounting evidence of the benefit of CGM in all people with type 2 diabetes, a recent article in Nature Reviews describes specific CGM strategies for 3 distinct groups.
#1 People with type 2 diabetes at diagnosis / early disease:
- It is recommended to use CGM for 14 days to establish an initial glucose profile and to provide education on how life style changes influence glucose levels.
#2 People with type 2 diabetes on insulin or sulfonylurea:
- Continuous CGM access is advised to prevent hypoglycemia and effectively manage hyperglycemia.
#3 People with type 2 diabetes not on insulin:
- Intermittent CGM use, suggested every 3 months, supports ongoing education on glucose profiles and the impact of medications.
In an era where cost-effectiveness remains a key concern, the application of CGM in people with type 2 diabetes not on insulin has been a topic of significant discussion.
At ATTD2024 prof Seidu (University of Leicester, UK) advocated for intermittent CGM use as a cost-effective strategy that balances expense with successful diabetes management.
This approach aligns with studies showing that intermittent CGM use can still lead to substantial improvements in HbA1c levels, promoting significant behavioural change and delaying the progression to insulin dependency.
Conclusion
As CGM technology continues to evolve and integrate more seamlessly into the lives of people living with diabetes, its implications for improving long-term health outcomes cannot be overstated.
The data presented at ATTD2024 underscores not only the life-saving potential of CGMs but also points to their broader applicability beyond people using (intensive) insulin treatment.
To continue exploring the transformative power of CGM technology and stay updated on the latest advancements in diabetes management,
I encourage you to grab our newly crafted comprehensive overview on current CGM systems.


This 2-page PDF offers in-depth comparisons and analyses, empowering you with the knowledge to tailor personalized diabetes care strategies for your patients.
Download your copy now and embark on a journey towards optimized care and improved quality of life.
Embrace the power of technology to transform the future of diabetes management—one glucose reading at a time.
Kind regards,
![]()



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}